
Founder and CEO of Memory Lane TV, Alban Maino is a media producer devoted to integrative health. After several years of product development, he launched this streaming media service, which provides therapeutically designed content that supports the well-being of individuals living with memory loss. Originally from France, Maino is also a US citizen and has just been nominated as Honorary French Consul, representing French culture and promoting economic development in his home state of Maine. He defines himself as a world citizen.
Dan Cohen: How did you decide to create this visual approach to improving well-being for people with dementia?
Alban Maino: When my grandmother was affected by dementia, I searched and searched for a tool, a medicine, something to help manage her symptoms, but I found that there were no effective options available. So, I delved into the published research and discovered decades of interventions and investigations into sensory stimulation on memory. Eventually I was able to leverage my media background—I’m a filmmaker and film producer—and construct some sensory simulation tools based on that research that helped with my grandmother’s symptoms. This was the genesis.
When I moved from France to the United States ten years ago, I was lucky to win a seat at the most prestigious accelerator program in the world, MassChallenge in Boston, and it allowed me to kickstart my venture, and that is when I heard of your similar work in the music field and Alive Inside.
DC: How is Memory Lane TV being used today?
AM: It’s very straightforward. I knew we had to develop something that would be technologically very simple and straightforward—It’s like Netflix on steroids! But that’s the only similarity, to basically download a media streaming app from any of the platforms stores. You click one button, and then you can navigate through the various collections that we have designed and start to enjoy our programming, or you can let the 24/7 pre-programed linear channel and follow the rhythm of the day.
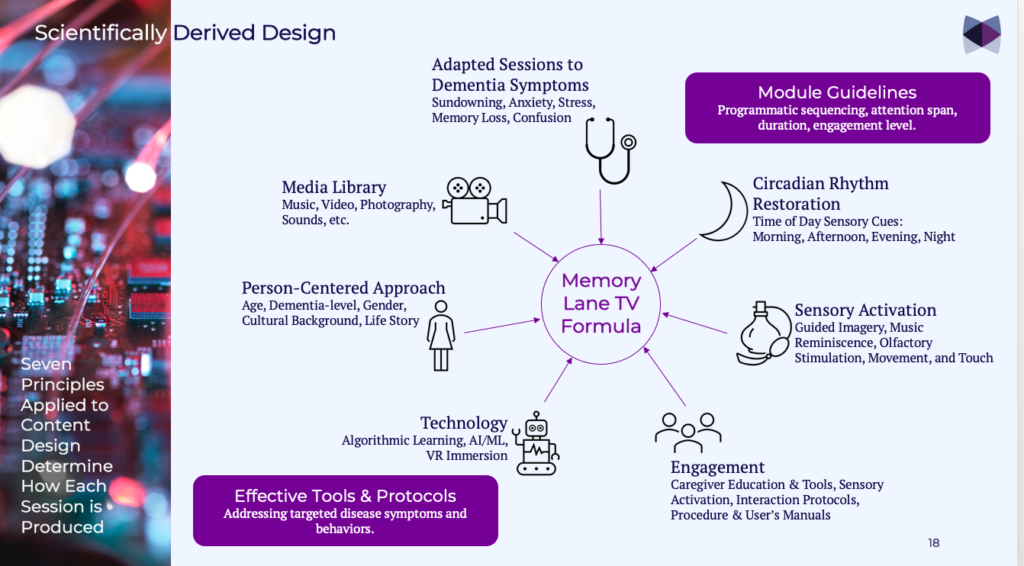
There are two ways of using it. When you register, we personalize and customize the content. You start by filling out a very quick survey, who the user is, where they were born, what type of music they like, and what type of environment is the most familiar in their personal history. We even ask questions about olfactory stimulation, what type of smells they like. Based on that we put together a personalized watch list that will really resonate and help caregivers manage different symptoms at different times of the day. It is a very person-centered approach.
And the second way, most likely in institutions, it can also be used as a television linear system, replacing regular television, which can be anxiety producing, with a very safe place. On the app, you can navigate and select from a variety of engaging short films (averaging 26 minutes, the attention span we measured during product development). Videos are also organized by time of day and level of engagement, following the circadian rhythm to address different needs throughout the day. Sometimes one needs to be engaged, at other moments we need our users to relax, or redirect their attention to a quieter place.

DC: Has there been research done on your approach?
AM: Absolutely. We are building on pre-existing research focused on the impact of sensory stimulation. We create a scientifically designed film montage with elements of music, soundscapes, video sequences, and still images to induce a variety of responses in the viewer, such as anxiety stress-reduction, re-grounding to combat sundowning, increased appetite, improved engagement, memory activation, as well as other positive benefits. Caregivers also benefit.
Initially we worked with geriatric physicians and occupational therapists in France. We quickly realized that media stimulation had wonderful potential as an additional caregiver tool. We did our own internal research, and we started to work with the Benson-Henry Institute for Mind Body Medicine at Massachusetts General with Dr. Herbert Benson, the famous researcher of the relaxation response. We discovered that the relaxation response that we were observing was actually a very studied effect and started to work with people that didn’t have any memory loss, people that have early onset dementia, and then moved on through a lot of nursing homes with memory care units.
We started documenting the effect by pairing students with one elder and gathering data about the efficacy of our intervention and how we could even enhance it. We continue to expand our research efforts in New England and are about to offer access to our intervention to all nursing homes in Maine through the Maine Dementia Coalition.
Three Main Benefits of Memory Lane TV
DC: From a nursing home perspective, what outcomes would be most noticeable to direct care staff?
AM: There are three main benefits in long-term care or at home: It increases respite opportunity. It decreases stress and anxiety. It improves interaction with a person for whom they are caring. All that increases productivity and staff quality of care but also offers a hedge to institutions that use our innovative and evidence-based, non-pharmacological intervention.
Unlike regular television, which really can exacerbate the very symptoms that our approach is designed to combat, all of our content is plot free and non-character dependent, so it’s not editorial. It’s not entertainment—yet it is entertaining! Think of it as a therapeutic tool designed to achieve symptomatic relief related primarily to anxiety and stress. When you have a panic attack or you’re dealing with sundowning syndrome, medication and psychotropics can be useful but will not have an immediate effect. We use different ways to redirect attention. Music and personalized playlists can achieve that. I’ve seen music work miracles.
Residents are not engaged in facilities, because programs are not adapted to the pathology and do the opposite of what our programs are designed to induce. People might think we’re magicians when they understand how to use the programs to manage specific behavioral symptoms; we’re just using tools. Dr. Oliver Sacks described it 30 years ago in Musicophilia, and mentioned the importance of music, for example, for people living with dementia.
We’re able immediately to relieve the anxiety, temper panic attacks of people who would normally create additional confusion in the environment that can easily propagate. That allows the environment to stay quieter. Productivity is enhanced. We have occupational therapists that have really enjoyed using our program because a lot of people are often left behind in nursing homes. Not everybody can be wheeled to activities or even have the capacity to follow activities. Throughout the day this is an extra tool.
Of course, we DON’T want people to sit in front of television! No one wants that. We know there is a lack—COVID has exacerbated that—of human resources to address the needs of our elders. This is an extra tool in staff’s toolbox to increase nursing home productivity while increasing social engagement at a really low cost.
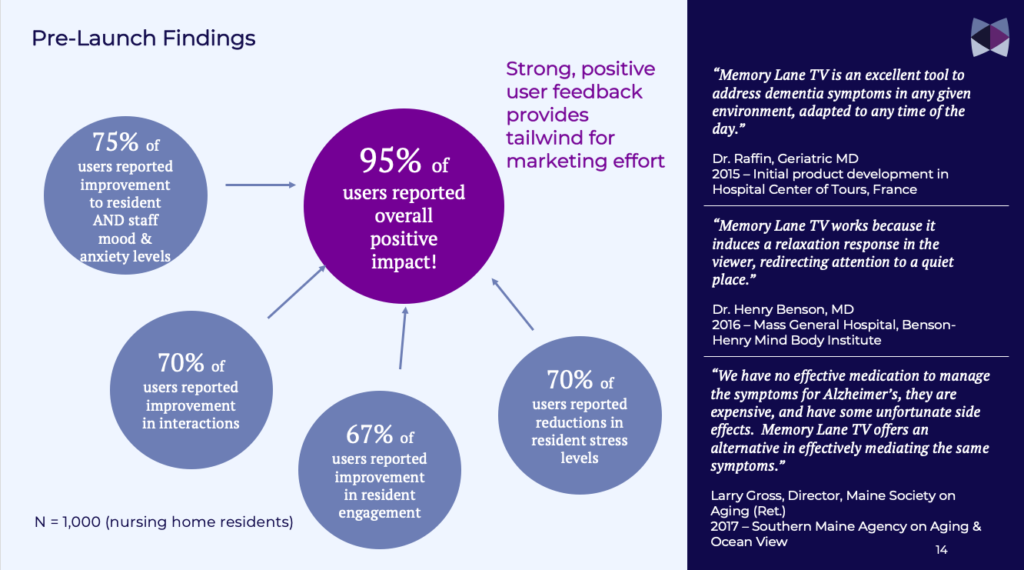
We recently produced a white paper that addresses the importance of multisensory stimulation and that includes the results of some of our research, which shows that we can reduce anxiety and stress considerably (as high as 80 percent sometimes) when properly using our programming. The science of cinematic perception, the reason why we all enjoy going to the movies, can be applied in care to induce specific positive outcomes: joy, smiles, happiness, reminiscence of positive and feel-good stories. It’s not brain science, but we can help rewire the brain for a moment. We can talk more about that if you want.

DC: When you say “increases respite opportunity,” what do you mean?
AM: One of the scariest statistics that I have read about dementia and Alzheimer’s disease is that 63 percent of caregivers will die during their time providing care, with many family caregivers dying an average of two years before the Alzheimer’s patient for whom they care. The emotional and logistical toll is actually bigger on the care partner and the caregivers. In the later stages of the disease, they have to do everything, which takes a huge emotional toll. I’m not talking only about organizing the care, but also staying connecting with their loved one.
Respite is a fundamental element to diminish stress and anxiety. How do we achieve that? With the help of the very essence of the programming that we produced. Our programming includes what I named “dreamscenes,” a sequence shot that last one to three minutes. They’re not character-dependent. They have no plot. But there IS a story. Viewers start dreaming, redirecting their attention as the cinematography takes you to a nice, quieter place, sort of a media meditation stimulation. Guided imagery is a science, by the way, and so is cinematic perception.
The attention span we’ve measured for our films averages 26 minutes. Beyond that we start losing people. So we take them on an arc. It might be used to help get someone excited for lunch, in the afternoon we get them to engage through quizzes and interactive games, and when we need more respite, we take them on a journey with our medleys, towards the end of the day, and our medleys uses that cinematic perception. Why do we love to go to the movies? Why do we enjoy those Netflix shows so much? Depending on the type of film you like, it induces something that makes you laugh, makes you calm, makes you happy or sad.
We use this, but we only focus on the positive, on the respite, and on the quiet impact that cinematography can have on you. I wish care partners could take everyone in the forest for an enjoyable walk or riding along the coast of Maine, but the reality is that most of them stay in their confined environments. We have the luxury of taking walks or, if like me you live in Maine, just to sit in front of the ocean after a long day creates inner peace, a moment of mindfulness that is extremely soothing for me as I grew up by the water. But not everybody can do that, especially when you’re in a nursing home. So we can help by bringing the outside, inside.
Personalized Video Content for Easier Transitions Through the Day
DC: To what degree is the video content personalized? You learn about the person, what they like, so it’s like a music playlist, but instead it’s a video playlist? Also, are all of your videos accompanied by music soundtracks?
AM: We have soundscapes in every single one of our videos. Sometimes we use ambient and natural relaxation sounds when we’re trying to bring about a calmer respite, drones or specific original music, as sometimes it’s good to fall asleep or rest or meditate. Other times we want people to be really engaged. Then we need to customize and personalize the content and increase the beat per minute.
When you register at Memory Lane TV, we create the user’s profile. Based on the answers—where you were born, how old you are, what is the name of your caregiver, what pets you may have had, where you grew up—we create a personalized watch list for you to begin your journey. If you grew up in Montana, it’s very different than if you grew up on the coast of Maine so we tailor the scenery to what’s familiar, it then resonates almost instantly. In Maine, for example, one of our most popular films is the Fryeburg Fair, an institution that is almost 100 years old that every Mainer has attended at least once. It is so much fun, and our cameras show you things you might be oblivious to, so it’s even more fun!
Not only can we customize and use our content to create a specific watch-list, but we will soon also be able to use the personal media of the family, favorite music, to create a film that will combine two, three, or four senses in one single video that will be part of a very intimate and personalized journey. What does that do? It tremendously increases the quality interaction between the care recipient and the care partners. You know the importance of personalized history, what you have described in Alive Inside as music illuminations. We all remember Henry and his reaction to his favorite song.
We create media illumination basically at different levels through our sense of smell, through media, through music, through soundscapes, through reminiscence. Memory Lane TV is like Music & Memory, yet applied to all the senses. Just the way the music of our childhood gives us the chills or re-connects us with long lost memories, we are building on that reminiscence by delivering a compelling combination of taste, smell, images, and music.
DC: One of the things I really love most on my phone is that it pulls up anniversaries or look-backs on vacations or photos grouped by family member (or pet!). I think this follows the same rules as you are since it’s not a story. It’s a narrative with familiarity. It lasts perhaps just 20 seconds, but it’s always a surprise, upbeat moment to my day.
AM: Hopefully, as mentioned, by the end of the year we’ll be able to even improve on that by mixing a person’s media with our relevant of images to create your own personal reminiscence film. Our contribution is both geographical and historical. If we know that the user was in her 20s in the 1960s, we can pull historical content out of that time frame, thanks to our partnerships with image archive banks, a snippet of five minutes of those special things and that will be mixed.
This is personalized cinema on steroids. We are bringing videos and music to the next level, thanks to technology. We experimented with VR as well and some of our films will be available in virtual reality environments, but we have learned that confusion can also arise from too much immersion, especially for our demographic, so one has to be careful.
For persons with dementia, we need to be sure the content is therapeutically designed. If not, there is the possibility that the experience will be very confusing in terms of understanding your environment. Each person’s response needs to be monitored.
Integrating Sense of Smell and Taste
DC: Please talk a bit about how you’re integrating other senses to enable positive well-being.
AM: Olfactory stimulation is a direct pathway to the brain. A rather expensive multi-sensory approach used by some nursing homes for decades for people with dementia and other pathologies are called Snoezelen rooms. The connection between memory and the sense of smell is well-documented in scientific research. But not only that, essential oils, when they’re carefully used, can induce all sorts of beneficial physiological responses in the user. Lavender will help you fall asleep, for example. Citrus will engage your appetite.
We partnered with two of the world specialists in that field who applied their experience and expertise to the field of dementia, Dr. Jennifer Stelter and Jessica Ryan, the founders of Neuroessence. Their research focused on dementia best practice and allowed us to create specific olfactory packages and to pair our films with different olfactory stimulation experiences. We have designed and are offering different tools to disseminate perfumes using vetted essential oils. You can either use them in a semi-public setting, through a diffuser, or with dots that you put on your clothes that you smell to add direct effect. This is the only part that is not digital in our intervention, but that’s one of the senses we address.
We’ve talked about audio and visual stimulation. We’ve talked about olfactory stimulation. The other two senses that we use are based on something that’s crucial to me and central to Memory Lane TV. How do you touch or not touch someone who has dementia? How do you use that essential element to bring more connection or to make people feel better? The same thing with food. Hygiene of the mouth is crucial and determinant of pathologies as well. It can lead to so many problems. Having proper food, using the taste of food in a very specific way is another focus of ours. Our collection of films includes a Caregiver Channel featuring leaders from the field such as Teepa Snow, the UCLA Alzheimer’s and Dementia Care Video series, the Lien Foundation or the DAWN method, an interactive training tool developed by Judy Cornish. Our Caregiver Channel serves as a resource to help care partners to understand how best to use multisensory stimulation in the context of dementia care.
A fun example of multisensory engagement for residents can involve making an apple pie. We designed a 26-minute film using music focused on showing how to do this. Care partners can bring tools to make an apple pie. And participants actually eat an apple pie after the film. You encourage people to talk about their own recipe, you keep everybody engaged! Spark interaction by pausing the film: “Hey, what do you think about homemade apple pie? Do you know about this, Margaret?” “No, I actually don’t know what they’re doing.” All of a sudden, we’re creating engagement. We’re all eating an apple pie. We are injecting apple scents into the environment, enhancing the quality of the experience. This is one of many examples of what we do with Memory Lane TV.
We know people with dementia and memory loss have auditory and visual impairments. It’s very important that we create that cinematic environment to optimize the impact. The bigger the screen, the better. Lower extraneous noise so we can fully immerse ourselves. Same thing with music and soundscapes. We educate the care partners to make sure that participants are close enough to the screen and speakers so that they can actually enjoy it. This is how we’re going to stimulate those senses. Because what you and I perceive might be very different. Teepa Snow is very good at explaining what it’s like to have dementia. You are having strange physiological movement. They see things that are not real or are real to them and not real to you. We took all that into consideration when we designed Memory Lane TV. What is good for us is even better for someone who lives with dementia and has direct impact also on the care partner.
An Alternative to Psychotropic Drugs and Their Side Effects
DC: What would you say to all those who are influencers in dementia care in terms of how important is it that we set up this kind of engagement for people who have dementia? And what can we do to help?
AM: Thank you for asking that question. Reducing stress and anxiety can lower the rate of psychotropic drugs and their side effects. If I break my arm, I go to the hospital, Western approaches to pathology are predominant and necessary, and pharma as we have seen during Covid has saved millions of lives, yet with what we’re dealing with—improving quality of life, offering more respite, dementia symptoms of memory loss and so on—there are so many really crucial, simple tools that people need to use that are non-pharmacological.
Our approach is still very innovative, and we need influencers, people in the world who are key opinion leaders, artist, scientists, filmmakers to relay our mission. And I will tell you why. I never wanted to add an additional financial burden to the care partners; their cost of care is already high, so maybe there are people out there who can help. Foundations, donors who want to help our cause and our communities. If you or any of your readers know someone that can help us by providing free access to everything that we are doing, this is one of the things I’d love to put in place. It was one of my dreams to make this available to the whole wide world, for free! But producing content is expensive, so I am always trying to think how we could make this work. There are 6 million Americans now affected by dementia and memory loss, 80 percent are at home, 55 million worldwide, and these numbers are exponentially growing with the aging of baby boomers.
Please contact us on our website, Memory Lane TV. Don’t take my word for any of it. Peruse our content, try it for free and then see how you could help, who you could help. One out of three of us will be in our lifetime affected by the disease.
DC: Is it downloadable in the Apple and Google App Store?
AM: Yes, all the app stores. And Memory Lane TV is free to try. The best way is to start is to go on our website. We have all sorts of videos that explain from A-Z in a very simple way how to use it and download it to your phone, to your tablet, to your computer, to your Roku, to your Amazon Fire Stick. It’s a very straightforward process.
DC: You mentioned that your service is available through many sources. Is this available for people at home?
AM: Another crazy statistic, scary statistic, easy to understand that I just mentioned, is that 80 percent of the people that are managing, or dealing with, symptoms of dementia or memory loss or Alzheimer’s disease when it’s diagnosed are still living at home. Caregivers are at a loss on every single level, and they need help. They don’t know how to deal with what’s happening and what is coming. They need to be educated on how to manage that journey. When you’re in nursing homes there is a lot of help available, and can be very expensive as we all know. You may be paying a lot of money for it, nurses, CNA’s, occupational therapists, doctors and all sorts of things depending on the level and quality of care that you’re getting there. At home you don’t. My focus since the beginning of this project was to help people that were at home, just like me and my grandmother.
Eight years ago when I started to work on this project, technology for home use wasn’t available. But now, thanks to Amazon, Google, and all the other big players, we independent producers have a pipeline to deliver to everyone’s home wherever you are. It’s also available in the same way in nursing homes and memory care units everywhere because it’s the same tool. We use different distribution systems because we want to be able to penetrate and make that available widely. It’s basically extremely easy to use and very cost effective too. Our strategy and hope is that a lot of companies already in that space will deliver our content through their pipeline to offer an added value service to their users.
DC: Is there anything else you’d like to add?
AM: In this industry, we are probably the only one to integrate audio, visual, and olfactory stimulation by design. Other approaches may offer one or two, but certainly not all of those elements. Our content is scientifically and therapeutically designed to target specific behavioral and psychological outcomes from inception. It’s not merely plot-free, meaning not character driven, it is entertaining, yet should not be considered as only entertainment. It is a tool to effectively manage behavioral symptoms associated with memory loss and improve the quality of life through guided imagery and reminiscence. Our service is designed to be equally effective, accessible, and affordable both in home and professional settings. Any untrained informal care partner providing care in their homes can use this tool just as effectively as a professionally trained care partner in big care facilities. It’s very simple, so why not use it. Everyone can help someone with memory loss.